


You can schedule directly with us; no physician referral required
Your journey begins with a personalized consultation and full medical history review.
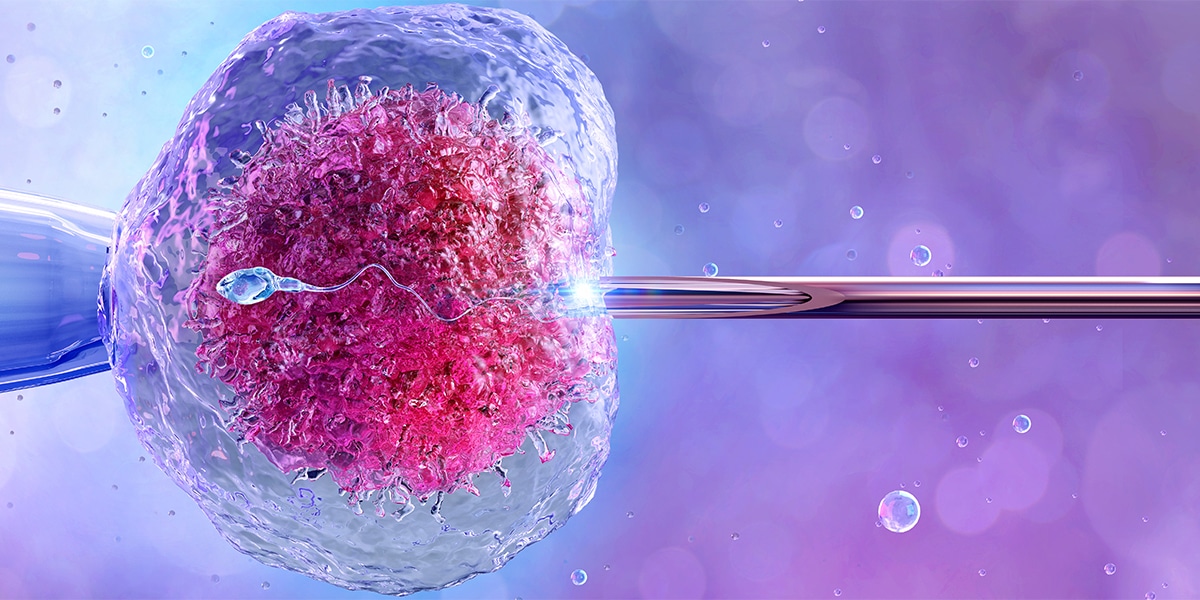
We offer thorough hormone, ultrasound, and cycle testing to uncover the cause of infertility.
Every patient receives a custom treatment plan based on results, goals, and budget.
We know fertility treatment is a big step – emotionally and financially. That’s why our dedicated financial counselor is here to help you navigate every option available. We accept most major insurance plans and also offer cash pay packages for patients who do not have insurance or prefer not to file treatment through their insurance provider.
Need additional support? Financing is available through trusted partners like Arc Fertility and United Medical Credit, giving you flexible payment solutions that fit your budget and your journey.

Every tiny miracle starts with hope.💕
#fina #HelpingFamiliesBuildFamilies … See MoreSee Less
0 CommentsComment on Facebook
Building families is our passion, and we truly love what we do. Thank you to our patient for sharing her experience.
#fina #HelpingFamiliesBuildFamilies … See MoreSee Less
0 CommentsComment on Facebook
We will call you by name at each visit because fertility care should always feel personal.💕 We're here when you're ready to start your journey.
#FINA #HelpingFamiliesBuildFamilies … See MoreSee Less
18 CommentsComment on Facebook